Author:

Longer lives did not begin with an already-modern health system. In recent work with Leon Huetsch and Dirk Krueger, we argue that economic growth first made basic health investments affordable and only later created the market that pulled frontier medical innovation into existence.
It is easy to think of modern medicine as a permanent feature of rich economies. Historically, though, it is surprisingly recent. For a 20-year-old in the United States, remaining life expectancy hovered at around 40 years until the mid-19th century. By 2020, it had risen above 60. Over the same long run, health moved from a marginal activity to a sector absorbing close to one fifth of spending.
That raises two linked questions. Why did adult life expectancy begin to rise well before the modern health sector took off? And why did that sector emerge so late, despite the obvious value people place on living longer?
In our paper, we build a quantitative model to answer both questions together. The central idea is simple: growth mattered twice. First, it let households spend more on basic health. Later, it created enough demand for longevity to redirect innovation towards medicine. That three-stage story helps explain not only why people live longer, but also why health spending rises so sharply once economies become rich.
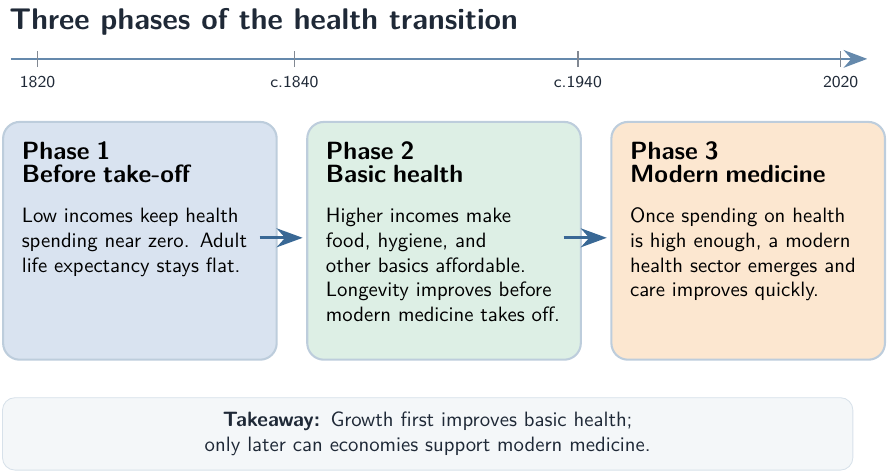
Three phases of longer lives
The first phase is stagnation. When households are poor and effective health goods are expensive, spending on longevity competes with basic consumption. In that environment, people find it optimal to spend very little on health, adult life expectancy stays broadly flat, and a modern health sector does not emerge.
The second phase begins when productivity growth pushes income up. At that point, households can start buying more of what we call basic health goods: better food, hygiene, and other simple investments that improve survival without requiring an advanced medical sector. A key implication is that longer lives do not start with hospitals, pharmaceuticals, or a large health industry. They begin earlier, when rising incomes make basic health investment feasible.
Only in the third phase does modern medicine take off. Once demand for longevity becomes large enough, it changes innovation incentives. Entrepreneurs direct more research and development towards health, medical quality improves, and a distinct modern health sector emerges. In our framework, that turning point comes only around the middle of the 20th century.
Rising medical prices are not the whole story
At first sight, the data create a puzzle. Measured health prices rise over time, which can make it look as if medicine simply becomes increasingly expensive. Our model suggests a more careful reading. The sticker price may rise even while the price of one quality-adjusted unit of health improvement falls.
That matters because a modern treatment today is not the same product as a treatment decades ago. Better diagnostics, more effective drugs, and higher-quality care all mean that part of the observed rise in medical prices reflects a better product rather than pure inflation. In the model, this distinction is central: the emergence of the modern health sector is driven by quality improvements, even if conventional price indices make health care look costlier.
What did modern medicine add?
Quite a lot, though not all of it. In the model, remaining life expectancy at age 20 rises by a little more than 10 years between 1940 and 2020. A crude way to value the modern health sector would be to assume that all spending on modern medicine simply disappears. Under that extreme exercise, almost 8.7 years would be attributed to the modern sector.
But that is too strong, because households would adjust if modern health goods were unavailable. In our preferred counterfactual, they adjust and shift spending towards basic health instead. On that basis, the modern health sector explains about 2.4 years of the post-1940 gain, or roughly one quarter of the total.
That is still a large effect. Frontier medicine matters. But the result is also a useful corrective to an overly narrow view of health policy. Most of the long-run improvement in adult life expectancy in the post-war
period still comes from broader income growth and the associated expansion of basic health investment. Modern medicine builds on that foundation; it does not replace it.
When public policy matters most
We also distinguish between two different ways government affects the health transition. The first is by supporting innovation. In our model, public spending on medical research and development during the Second World War plays a pivotal role in getting the modern health sector off the ground. Remove that intervention, and the sector barely emerges in the 1940s. By 2020, remaining life expectancy is slightly less than one year lower. Put differently, close to one tenth of the post-1940 rise in life expectancy can be traced to that early innovation push.
The second channel is public insurance and demand support. Medicare and Medicaid substantially raise the spending share of the modern health sector in the model, but they have only negligible effects on life expectancy in the model. That should not be read as a general verdict on those programmes. It reflects the narrower mechanism we study here: these policies mainly shift demand towards modern health goods, rather than directly changing survival.
What this changes for health policy
The broader lesson is that the history of longer lives is neither a pure growth story nor a pure medicine story. Growth improves health first by making basic investments possible. Modern medicine matters later, once demand is strong enough to sustain a large innovation-intensive sector. Public policy can matter at both margins, but it matters in different ways.
The right question is not simply whether health spending should be higher or lower. It is when policy should raise basic living standards, when it should support new medical technologies, and when it is mostly financing demand within an already mature sector. Understanding why people live longer, and how policy can extend that progress, requires thinking about the evolution of the health sector rather than only its current scale
Author: Alexander Ludwig